clinical genetics
AI DNA Analysis vs Genetic Counseling
AI DNA analysis and genetic counseling answer different questions. Learn when each fits, where the line is, and how to use them together.
Sebastian Thorp · May 7, 2026 · 7 min read

In short
AI DNA analysis and genetic counseling are not competing products. They sit at different points in the patient journey, answer different kinds of questions, and use different evidence. AI tools handle context-aware education and pre-visit preparation well. Certified genetic counselors handle clinical risk assessment, family planning, and decisions with consequence — and remain irreplaceable for those. The question isn't which one to use. It's which one is right for this question, and how to use them together.
What a genetic counselor actually does
A certified genetic counselor (in the US, typically credentialed by the American Board of Genetic Counseling; in the UK and Norway, registered through national professional bodies) is a clinical professional with a master's-level education in medical genetics, psychosocial counseling, and risk communication.
The work is broader than most consumers realize:
- Family-history risk assessment — building a multi-generation pedigree, identifying patterns suggestive of inherited cancer syndromes, cardiac conditions, or rare disease
- Test selection — which genetic test (if any) is appropriate, given the question being asked, family history, and clinical context
- Result interpretation in clinical context — what a positive, negative, or variant-of-uncertain-significance result actually means for this patient
- Reproductive counseling — carrier-status implications for family planning, prenatal testing options, donor selection
- Coordination of clinical care — referring to specialists (oncology, cardiology, neurology) when a finding warrants it
- Psychosocial support — helping a patient process information that is often emotionally weighted
Crucially, this is regulated clinical work in most jurisdictions. The training, scope, and accountability are not equivalent to "an app that explains variants."
What AI DNA analysis does well
AI DNA analysis sits in a different lane. The tools are educational and informational, designed for pre-clinical questions and ongoing context-aware learning.
The category does well at:
- Synthesizing your consumer DNA file into a readable narrative — taking 600,000+ variant calls and producing a prioritized report instead of a spreadsheet
- Personalizing against your reported context — supplements, symptoms, habits, goals all shift how a finding gets framed (how this works)
- Citing primary sources — every claim should trace back to ClinVar, PharmGKB, GWAS Catalog, or peer-reviewed literature
- Findings-grounded follow-up — answering specific questions later, with citations, grounded in your findings (more here)
- Pre-visit preparation — surfacing the variants worth discussing at a clinical appointment, with the evidence levels attached
What it doesn't do — and shouldn't claim to do — is clinical interpretation, diagnosis, or risk decisions with consequence. That is the line.
Where they overlap (carefully)
There's real overlap in the information layer — both can explain what a variant is, what evidence supports its association, and what the literature says about typical effects.
The non-overlap is the decision layer: what to do about it, in your specific clinical situation, given your family history and your medical context. That's counseling. AI tools should not — and serious AI tools do not — operate there.
A useful frame: AI DNA analysis is content. Genetic counseling is decision support with clinical accountability. The same fact about MTHFR can be educational background in one context and a treatment-influencing data point in another, and the difference is who's responsible for the next step.
When AI DNA analysis is the right tool
The category fits these jobs well:
- You have a consumer DNA file and want to understand the actionable parts of it without reading 50 PubMed papers. Educational use, lifestyle context, supplementation choices.
- You're starting a new medication and want to bring informed questions to your prescriber. Drug-gene interactions (PharmGKB Levels 1A–2B) are well-suited to AI synthesis. The decision still belongs to your prescriber.
- You want to prepare for a clinical appointment. Identifying which findings are worth raising — with the evidence levels attached — saves visit time.
- You want ongoing learning. Variant interpretation evolves. A grounded chat lets you re-engage with new questions as they arise, without booking another appointment.
For these uses, an AI DNA tool is faster and more economical than scheduling a counseling appointment, and the appointment may not be the right next step at all.
When genetic counseling is the right tool
The category that AI cannot substitute for:
- Family history suggestive of inherited syndrome. Hereditary breast / ovarian / colorectal cancer, cardiomyopathies, hereditary connective-tissue disorders, neurodegenerative conditions with familial patterns. These need pedigree analysis and clinical-grade testing decisions, not consumer-chip interpretation.
- Family planning involving carrier-status concerns. Consumer carrier reports cover a small subset of the relevant variants and don't address reproductive decision-making with the rigor required.
- A specific clinical question with consequence. "Should I have prophylactic surgery?" "Should my children be tested?" "Should I change a planned medication based on this finding?" These are clinical decisions with clinical accountability.
- A diagnostic odyssey. When something clinically unclear has been going on for years and a genetic explanation is being considered, you need a clinician who can integrate genetic testing with a full clinical workup.
- Variant-of-uncertain-significance (VUS) interpretation in clinical context. Consumer chips don't typically return VUS results, but if you have one from a clinical-grade test, interpretation requires more than a database lookup.
In each case, the move is to a credentialed counselor (or geneticist) — not a better AI tool.
How to use them together
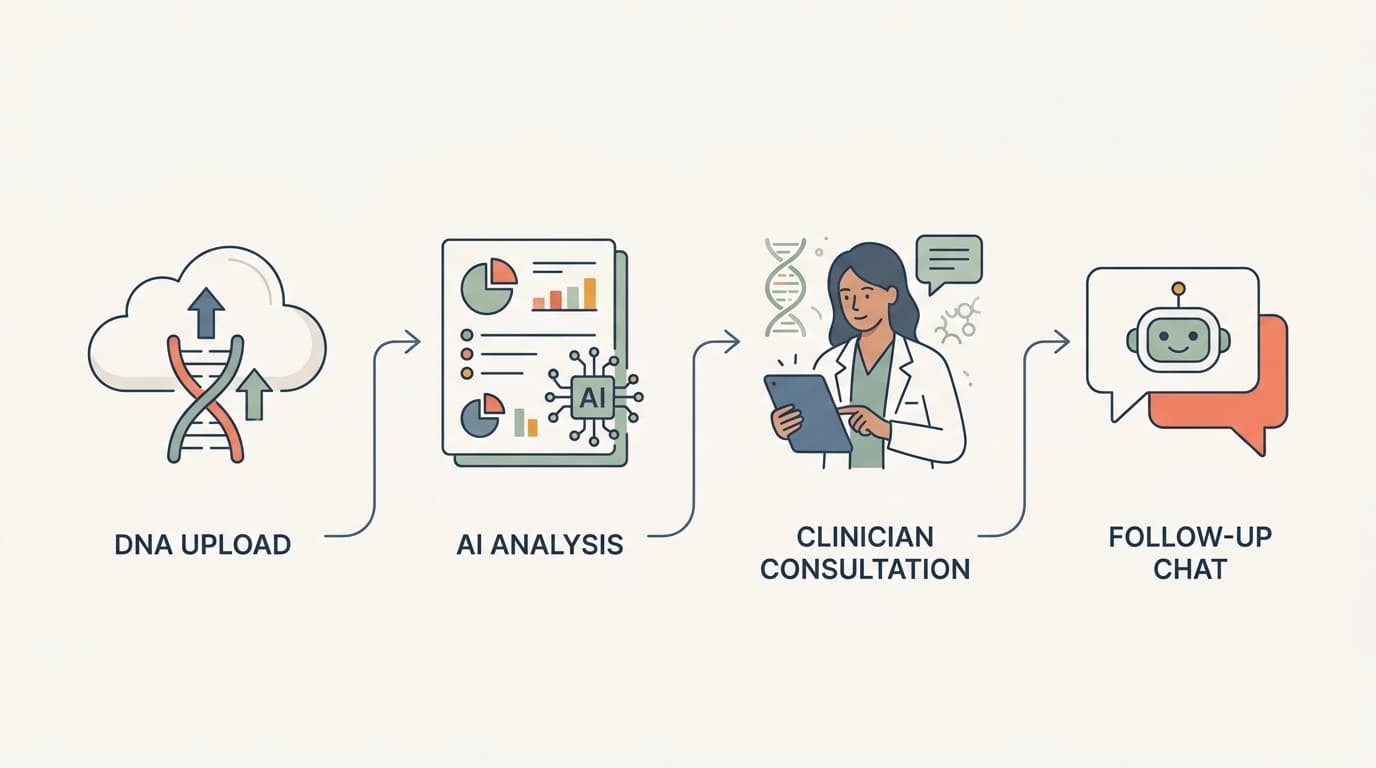
The honest answer is most useful when both tools work in sequence.
Pre-visit: an AI DNA analysis tool turns your consumer DNA file into a structured, prioritized list of findings worth discussing. You arrive at the appointment with the specific questions formed, evidence levels attached, and your own context (supplements, symptoms, goals) already mapped.
During the visit: the counselor brings the clinical interpretation, family-history integration, and decision support that AI tools are not equipped for. The structured pre-visit notes save time and let the conversation focus on the parts that matter.
Post-visit: an AI DNA analysis chat lets you ask follow-up educational questions as they come up — the kind of questions that would be wasteful to schedule another appointment for. "What was the significance level on that BRCA1 result the counselor mentioned?" is a question that doesn't need clinical context; it needs reliable retrieval against the cited evidence.
This isn't AI replacing a clinician. It's AI doing the educational work between clinical interactions, so the interactions can do their actual job.
What to look for in either tool
Whether you're choosing an AI DNA analysis tool or a genetic counselor, the same underlying signal applies: credentials and citation discipline.
For an AI tool: does it cite primary sources for every factual claim? Does it acknowledge uncertainty? Does it refuse to diagnose? Is the raw genotype file kept out of the LLM context? (What good privacy posture looks like.)
For a genetic counselor: are they credentialed by a recognized professional body? Do they have experience in the specific condition area you're concerned about? In the US, the NSGC's Find a Genetic Counselor directory is the standard search. In Norway, the medical-genetic units at university hospitals (Oslo Universitetssykehus, Haukeland) handle clinical referrals.
The two are complementary professionals, in two different professions. The mistake is treating them as substitutes.
What GenoSight's role is — explicitly
We are an AI DNA analysis tool. We are educational and informational. We are not a clinical diagnostic test, not a substitute for genetic counseling, and not a substitute for clinical-grade testing when that's what's appropriate.
Where the user-facing posture lands: GenoSight surfaces actionable findings from your consumer DNA file, cites every claim, includes a findings-grounded chat for follow-up education, and routinely directs users to a healthcare provider or genetic counselor when the question warrants clinical handling. The medical disclaimer on every report and chat session is not legal boilerplate; it's an honest statement of where the line is.
Bring data to your next appointment
Upload your raw DNA, get a prioritized report with primary-source citations, and walk into your next clinical visit with the right questions formed. 250 free signup credits.
Medical disclaimer
GenoSight provides educational information about your genetic data. It is not a medical diagnosis, treatment, or cure. It is not a substitute for genetic counseling or clinical-grade genetic testing. Variant associations describe statistical relationships, not deterministic outcomes. Always consult a qualified healthcare provider or certified genetic counselor for decisions with clinical consequence.
Key takeaways
- AI DNA analysis and genetic counseling answer different kinds of questions. They are complementary, not competing.
- AI tools handle education, context-aware synthesis, citation-backed Q&A, and pre-visit preparation well.
- Genetic counselors handle clinical risk assessment, family-planning decisions, diagnostic interpretation, and decisions with consequence.
- The most useful pattern is sequential: AI for pre-visit prep, counselor for clinical decisions, AI for post-visit follow-up education.
- For finding a counselor, professional bodies (NSGC in the US, hospital medical-genetic units in Norway/UK) are the credentialed sources.
- For evaluating an AI DNA tool, look for primary-source citations, uncertainty acknowledgment, refusal to diagnose, and good privacy posture (raw DNA never sent to the LLM).