MTHFR
Methylation vitamins: a genetics-first guide to methylated B-complex supplements
Methylated B-vitamins help if you carry an MTHFR variant. Here's how to read your 23andMe genotype to decide if 5-MTHF is worth the extra cost.
Pernille · April 30, 2026 · 7 min read
Quick takeaway
Methylation vitamins are B-complex nutrients — folate, B12, B6, riboflavin — that fuel a chemical reaction your body runs billions of times per second. Whether you should take the methylated (pre-activated) versions or the cheaper synthetic forms depends mostly on one thing: your MTHFR genotype. This guide explains the cycle in plain language, shows when methylated forms actually help, and how to read your 23andMe or AncestryDNA file to make the call.
What methylation vitamins are — and why they matter
Methylation is the biochemical process of attaching a single methyl group (CH₃) to another molecule. It happens roughly a billion times per second across your body and is required for DNA repair, neurotransmitter synthesis, detoxification, and energy production.
The "methylation vitamins" are the B-vitamins that act as cofactors in this cycle: folate (B9), B12 (cobalamin), B6 (pyridoxine), riboflavin (B2), and the choline family. Without enough of any one of them, the cycle slows down.
A common point of confusion: methylation vitamins and methylated vitamins are not the same thing. The first is a category — any B-vitamin that supports methylation. The second is a form — the pre-activated version of that vitamin, like 5-MTHF (methylfolate) instead of folic acid, or methylcobalamin instead of cyanocobalamin.
The whole methylated-versus-synthetic decision usually rests on one variant in one gene: MTHFR. (We have a deeper explainer on MTHFR covering what "compound heterozygous" actually means and why the variant gets so much hype.)
The methylation cycle, in plain language
The core loop is the one-carbon cycle. Methionine donates a methyl group and becomes S-adenosylmethionine (SAM-e), which hands that methyl group off to whatever needs it — DNA, neurotransmitters, hormones. The leftover SAH then converts to homocysteine, which has two fates: get re-methylated back into methionine, or be cleared via the transsulfuration pathway into glutathione.
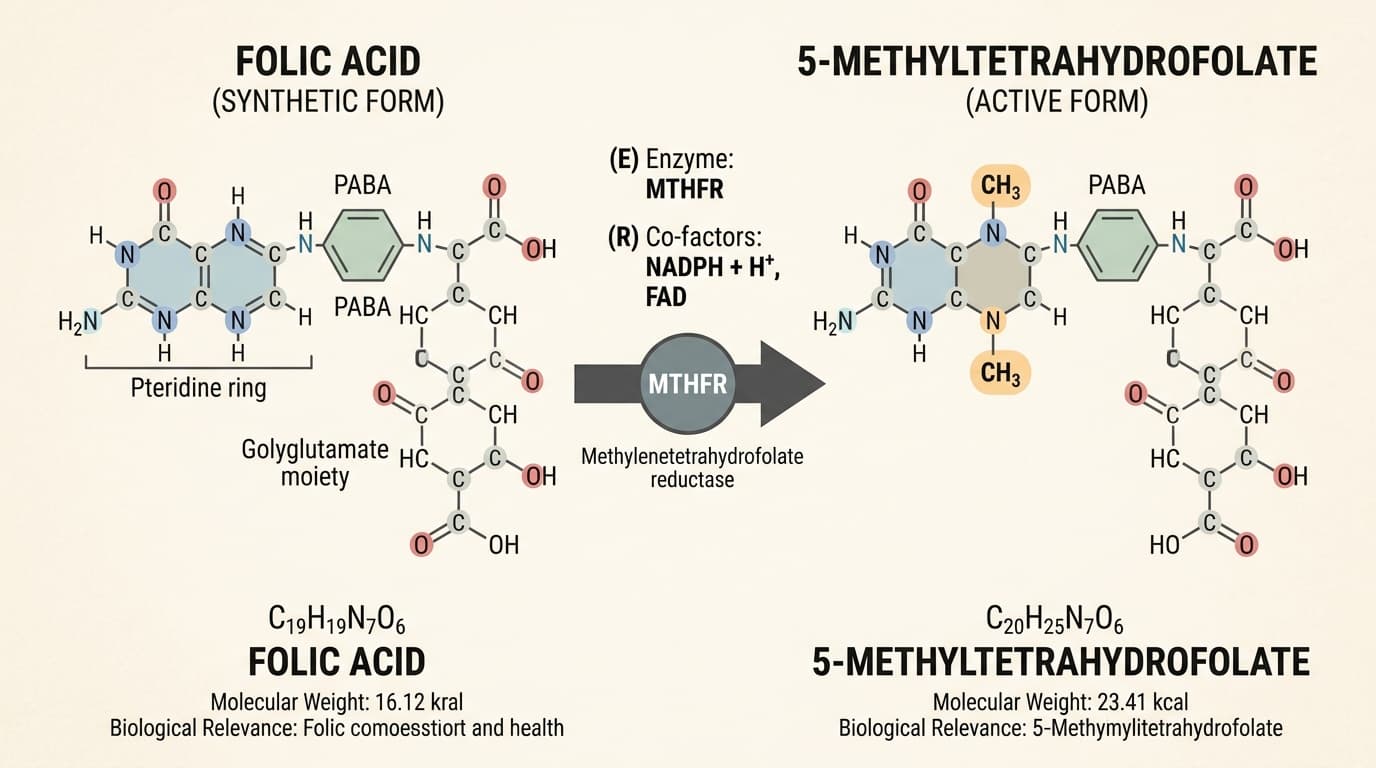
Re-methylation is where folate and B12 do their work. The MTHFR enzyme (methylenetetrahydrofolate reductase) converts dietary folate into 5-methyltetrahydrofolate — the active form your cells actually use. Methionine synthase (MTR) then uses that 5-MTHF, plus B12 as a cofactor, to recycle homocysteine back to methionine.
When MTHFR works at full capacity, the cycle hums. When it doesn't, homocysteine climbs above the normal 5-15 µmol/L range, folate utilization drops, and downstream methylation reactions get short-changed.
When methylated B-vitamins help — and when they don't
Two MTHFR variants matter clinically. The big one is C677T (rs1801133), discovered by Frosst et al. in 1995. The smaller one is A1298C (rs1801131).
| MTHFR genotype | Approx. enzyme activity | Population frequency | Methylated forms typically helpful? |
|---|---|---|---|
| C677T heterozygous (CT) | ~60–70% of normal | ~30–40% in European ancestry | Often, especially with elevated homocysteine |
| C677T homozygous (TT) | ~30–40% of normal | ~10–15% in European ancestry | Yes — strongest evidence base |
| A1298C heterozygous/homozygous | ~80–95% of normal | ~10–32% by ancestry | Debated; smaller effect size |
| Wild type (CC, AA) | 100% | Most common | Synthetic folic acid is fine |
A 2021 review summarized it well:
Methyl nutrients include folates (vitamin B9), riboflavin (vitamin B2), cobalamin (vitamin B12), pyridoxine (vitamin B6) and choline (vitamin B4), as well as methionine and betaine.
— Łoboś & Wojtczak, J Appl Genet 2021
There's a meaningful counterpoint: over-methylation is a real side effect. People with slow-metabolizer COMT variants — which break down dopamine and norepinephrine more slowly — sometimes report anxiety, irritability, or insomnia when they start methylated B-complexes. The fix is usually a lower dose, not a different supplement.
How to find your MTHFR variant in 23andMe / AncestryDNA / MyHeritage data
If you've already tested with one of those services and downloaded your raw genotype file, you can find your call directly:
- MTHFR C677T = rs1801133. The risk allele is T. Genotypes appear as
CC(wild type),CT(heterozygous), orTT(homozygous). - MTHFR A1298C = rs1801131. The risk allele is C. Same convention:
AA,AC,CC.
23andMe's strand orientation can swap which allele appears in the call (an AG may be reported at one variant where another lab reports CT). Bidirectional genotype matching is non-trivial. GenoSight handles strand orientation automatically and contextualizes the result against your full 9-domain health profile, so you don't have to manually translate between dbSNP, 23andMe, and AncestryDNA conventions.
Methylated vs synthetic B-vitamins: a side-by-side
The price difference between synthetic and methylated forms is usually 2–4×. Whether that's worth it comes down to which form your body actually uses without modification.
| Vitamin | Synthetic form | Methylated/active form | Who benefits from the active form? |
|---|---|---|---|
| Folate (B9) | Folic acid | 5-MTHF / L-methylfolate | MTHFR C677T carriers, especially TT |
| B12 | Cyanocobalamin | Methylcobalamin (or hydroxocobalamin) | MTR / MTRR variant carriers; vegans with low absorption |
| B6 | Pyridoxine HCl | P5P (pyridoxal-5-phosphate) | People with reduced PNPO activity |
| B2 (riboflavin) | Riboflavin | Riboflavin-5-phosphate | Most people convert riboflavin fine; matters mainly for MTHFR-aware dosing |
The B12 picture deserves a footnote. Cyanocobalamin carries a tiny cyanide group your liver removes during activation. For most people that's a non-issue. For smokers, who already have elevated cyanide exposure, methylcobalamin or hydroxocobalamin is the safer default.
A note on dosage: the DRI for folate is 400 µg DFE for adults, with an upper limit of 1,000 µg from synthetic sources to avoid masking B12 deficiency. Methylated folate doesn't have the same masking concern, but you still want to start at the lower end of the studied range.
How GenoSight personalizes your methylation supplement plan
GenoSight's analysis engine reads the variants that actually matter for methylation — MTHFR, MTR, MTRR, COMT, CBS — directly from your raw genotype file. That alone isn't new: there are free tools that look up the variant calls. (If you're curious about the data sources we use and don't use, see where GenoSight's insights come from.)
What's different is the synthesis. The engine cross-references your variants against the nine health profile domains you fill out during onboarding (current supplements, symptoms, labs, family history, and so on). A C677T homozygous result reads differently for someone already on methylated B-complex with no symptoms than for someone with elevated homocysteine and chronic fatigue. The full breakdown of what lands in your finished report is in what's in a GenoSight report.
The findings-grounded chat is the second half. After the report, you can ask follow-ups like:
- "Why methylcobalamin and not cyanocobalamin in my case?"
- "What dose makes sense given that I'm already taking SAM-e?"
- "Should I retest homocysteine before or after starting?"
Each answer is grounded in your specific findings, not a generic FAQ.
Practical considerations before you buy
Five things worth knowing before you reach for a methylated B-complex:
- Look for third-party testing. Supplement quality is unregulated; products from USP, NSF, or ConsumerLab-verified manufacturers are a meaningfully better bet than house brands.
- Start low. Begin at the lower end of the studied range. Methylated folate at 400–800 µg is plenty for most people; some methylated B-complex products contain 1,000+ µg, which is more than necessary unless you have a documented deficiency.
- Check interactions. Methylated B-vitamins can interact with SAM-e, certain SSRIs, methotrexate, and some anti-epileptics. Pull up your medication list before you add anything new.
- Get a baseline. A homocysteine test (often $30–60 out of pocket) before and after 8–12 weeks of supplementation tells you whether the protocol is working biochemically, not just whether you "feel better".
- Talk to your provider. Especially if you're pregnant, planning pregnancy, on prescription medications, or managing a chronic condition.
Medical disclaimer
GenoSight provides educational information about your genetic data. It is not a medical diagnosis, treatment, or cure. Always consult your healthcare provider before making decisions based on this information. Variant interpretation evolves; recheck periodically.
Key takeaways
Key takeaways
- Methylation vitamins (folate, B12, B6, B2, choline) are cofactors for a reaction your body runs billions of times per second — DNA repair, neurotransmitter synthesis, detoxification all depend on it.
- Methylated forms (5-MTHF, methylcobalamin) help most when you carry an MTHFR C677T variant — especially the TT homozygous genotype, which has roughly 30–40% of normal enzyme activity.
- Most people without an MTHFR variant do fine on synthetic folic acid; methylated forms add cost without clear benefit.
- Watch for over-methylation if you also have a slow COMT variant — anxiety, irritability, insomnia at standard doses point to dropping the dose, not switching products.
- GenoSight reads your raw 23andMe / AncestryDNA / MyHeritage file, contextualizes MTHFR + MTR + MTRR + COMT + CBS against your full health profile, and makes the genotype-aware recommendation explicit.