snps explained
What's in a GenoSight Report: The 6 Health Domains
A GenoSight report reasons about your genetics against six health profile domains. Here is exactly what each domain captures and why it changes the report output.
Sebastian · May 1, 2026 · 5 min read

In short
A GenoSight report isn't a generic gene lookup. Before any synthesis happens, an onboarding chat captures six health-context domains: demographics, symptoms, current stack, allergies, habits, and goals. The genetic findings are then interpreted against that context — meaning the same MTHFR variant may produce a meaningfully different recommendation depending on what's already in your supplement list and what you're trying to achieve. This walkthrough covers each domain, why it matters, and what gets asked.
Why context changes the output
Two people can carry the exact same variant and benefit from completely different framing. A C677T heterozygous result alongside a balanced diet, regular exercise, and no current concerns reads as a watch-and-wait finding. The same variant in someone reporting persistent fatigue who is already taking a B-complex with synthetic folic acid is a far more actionable item to discuss with a clinician.
Tools that don't capture context can't make that distinction. They produce the same paragraph for both people. (How that synthesis actually runs.) GenoSight's onboarding is built around the idea that the variant is half the data; the rest is who you are.
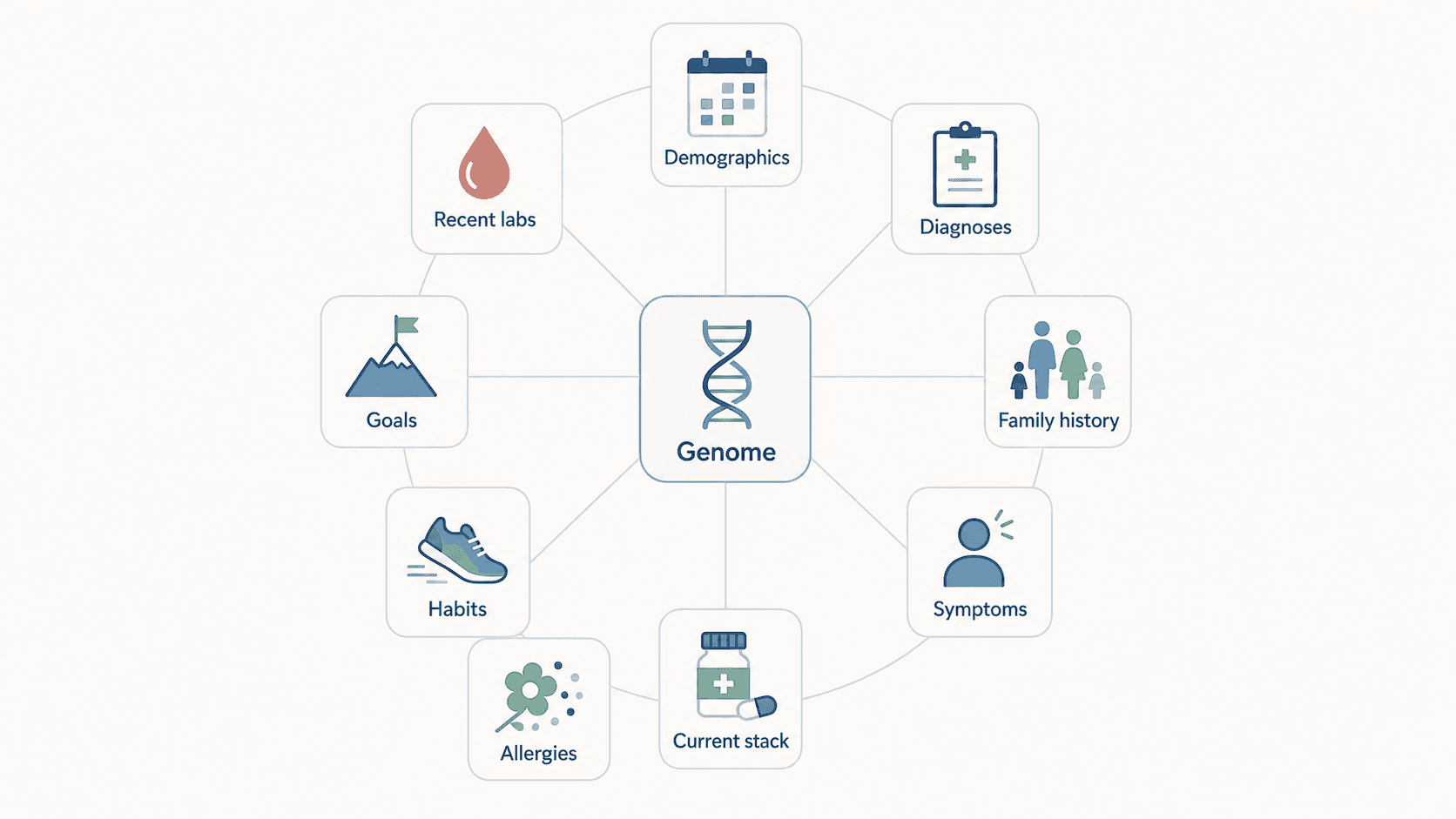
The six domains
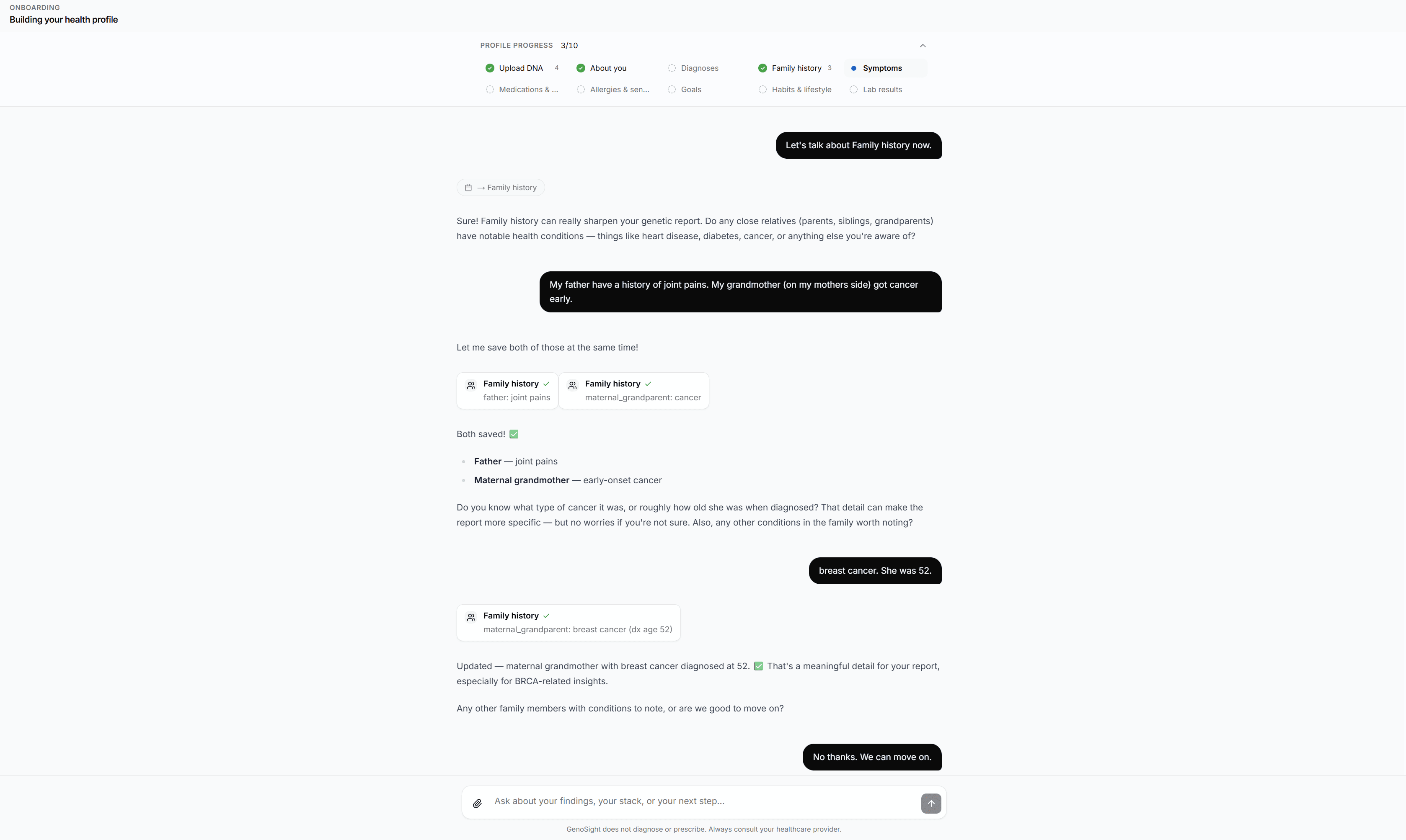
Each domain feeds into the synthesis prompt as structured context. None of them is a free-text dump — the onboarding chat asks targeted questions, and the answers get stored as typed fields the engine can reason about. Genosight does not collect medical diagnoses, prescription medication lists, family medical history, or laboratory values; those belong with your healthcare provider, not with a consumer-genomics service.
1. Demographics
What we ask: age, sex assigned at birth, ancestry (best estimate), height, and weight.
Why it matters: allele frequencies vary across populations, so "rare variant" needs a denominator. A SNP that's rare in European-ancestry cohorts may be common in East Asian cohorts, and the educational interpretation shifts accordingly. Body composition affects how some lifestyle-SNP findings should be read.
2. Symptoms
What we ask: current health concerns or symptoms you'd want the report to address.
Why it matters: symptoms guide the executive summary. If you mention chronic fatigue, the report looks specifically at variants relevant to mitochondrial function, B-vitamin metabolism, iron handling, and thyroid pathways. If you mention insomnia, the synthesis pulls in CLOCK, PER3, COMT, and ADORA2A findings.
3. Current stack
What we ask: supplements you're currently taking, with form where you have it.
Why it matters: this is the highest-leverage domain. A methylated B-complex finding reads completely differently for someone already taking 5-MTHF than for someone on synthetic folic acid. Stack-aware synthesis is what makes the report useful instead of theoretical. Genosight does not collect prescription medications.
4. Allergies
What we ask: food allergies and environmental sensitivities.
Why it matters: allergy information lets the report rule out specific suggestions (some methylated B-complexes are derived from corn, for example).
5. Habits
What we ask: typical diet pattern, sleep duration and quality, exercise frequency and type, alcohol intake, caffeine intake, smoking status.
Why it matters: lifestyle SNPs only translate into recommendations through the lens of current habits. A high-caffeine consumer with a CYP1A2 slow-metabolizer genotype gets a meaningfully different report than someone with the same genotype who already drinks decaf. ADRB2 exercise-response variants matter more if you're training; less if you're not.
6. Goals
What we ask: what you want to optimize for — performance, longevity, fertility planning, prepping for a clinical visit.
Why it matters: goals decide tone and depth. A "prepping for a clinical visit" goal triggers a clean PDF optimized for handoff to a clinician. A "longevity optimization" goal pulls in lifespan-associated findings that wouldn't otherwise be prioritized.
A worked example
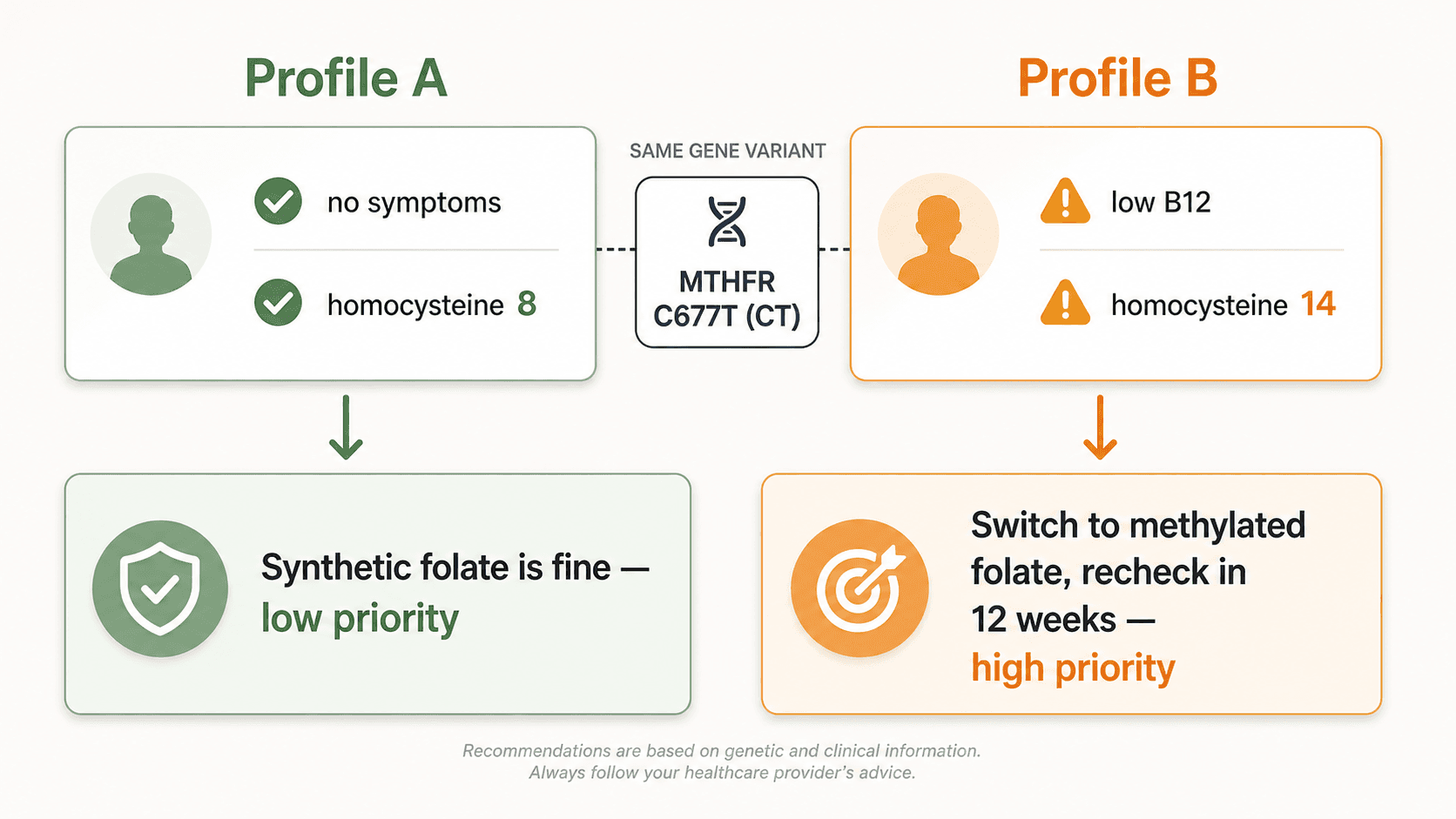
The same finding, two different reports:
Profile A. 34, female, balanced diet, regular exercise, no current concerns, no supplements. Carries MTHFR C677T (CT heterozygous).
The report: low-priority finding, brief mention. The educational note flags that folate-rich diet generally meets demand for heterozygous carriers without elevated homocysteine.
Profile B. 47, female, currently taking a generic B-complex with synthetic folic acid, lists fatigue and low energy in symptoms. Carries the same MTHFR C677T (CT heterozygous).
The report: higher-priority finding, prominent placement. Educational discussion of why a methylated B-complex form may be worth raising with a clinician, with a structured PDF section to bring to the conversation. No specific dosing, no diagnostic claim — just structured context for a real medical visit.
Same gene, same genotype. Different person. Different report.
What you don't have to provide
The onboarding is gated — every domain is optional except the bare minimum required for the engines to run. Reports get more useful as you fill in more, but you don't have to share anything you don't want to. You can update domains later and regenerate the relevant report sections.
Sensitive data is stored encrypted at rest with row-level security so each user can only read their own data. The raw genotype file is stored separately and is never sent to the LLM during synthesis — only the structured engine findings. (Full breakdown of how raw DNA data is handled.)
For the broader picture of how the report is produced — the parsers, the engines, and the synthesis pass — see what GenoSight is and how AI reads your DNA.
See your own report
Upload your raw DNA, fill in the 6-domain profile, and get a synthesis built around your specific context.
Educational only
GenoSight provides educational information about your genetic data. It is not a medical diagnosis, treatment, or cure. Always consult your healthcare provider before making decisions based on this information. Variant interpretation evolves; recheck periodically.
Key takeaways
- A GenoSight report reasons about your genetics against six health-context domains, not in isolation.
- The six domains: demographics, symptoms, current stack, allergies, habits, goals.
- We do not collect medical diagnoses, prescription medications, family medical history, or lab values — those belong with your healthcare provider.
- Same variant + different context = different framing. The MTHFR C677T worked example shows this concretely.
- The current-stack domain is the highest-leverage input — most educational notes only make sense relative to what you're already taking.
- Onboarding is gated; you only fill in what you want, and you can update domains later to refine the report.


